You are going to the gym. You are eating better but you are not losing weight. The scale has not moved in three weeks. This is not a willpower problem — it is a biology problem. Here is exactly what is happening inside your body and how to fix it.
4–6 wks
When most people hit their first fat loss plateau
500 kcal
Extra daily calories consumed on ultra-processed food diets vs whole food diets
7–9 hrs
Sleep needed nightly to keep fat storage hormones in check
The Real Question to Ask When Fat Loss Stalls
When you are exercising and eating right but not losing weight, the answer is almost never that you are not trying hard enough. It is that one or more biological systems in your body are actively working against fat loss — and no amount of extra effort fixes a biological mechanism problem.
You have probably read the standard advice already. Eat less, move more, sleep better, reduce stress. That advice is not wrong — but it skips the most important part. It does not tell you why these things stop fat loss at a biological level, which means you cannot identify which mechanism is actually causing your specific plateau.
This article is different. For every reason your fat loss has stalled, I am going to explain the exact mechanism — what is happening inside your body, why it happens, and what specifically breaks the cycle. As a fitness instructor and sports science nutritionist who has worked through this personally and with hundreds of clients, I can tell you that most plateaus have a clear, fixable cause once you understand the biology.
Important distinction before we start: This article covers fat loss, not scale weight. These are not the same thing. Your scale measures total body mass — fat, muscle, water, food in your gut, everything. Fat loss is specifically the reduction of adipose tissue. Many people are losing fat while their scale weight stays flat or even rises. We will cover exactly why this happens in the section on the scale.
Reason 1: Your Metabolism Has Adapted to Your New Calorie Intake
Metabolic adaptation is the single most common and least understood reason fat loss stalls. Your body is not broken. It is doing exactly what it evolved to do — surviving a food shortage. The problem is that your calorie deficit has been interpreted as a threat, and your body has responded by burning less.
How metabolic adaptation actually works
When you consistently eat below your maintenance calories, your body reads this as a famine signal. Several things happen simultaneously in response.
Your thyroid reduces the production of active thyroid hormone (T3), which is the primary regulator of metabolic rate. Your resting metabolic rate — the calories your body burns just to keep you alive — drops by as much as 15 to 25% in severe cases. Your body also becomes more efficient at movement, burning fewer calories to perform the same exercise you used to burn more calories doing.
The cause → effect chain
Sustained calorie deficit → body reads this as food scarcity → thyroid reduces T3 production → resting metabolic rate drops → you now burn fewer calories per day than you did when you started → the same deficit that worked in week 1 no longer creates a deficit in week 6
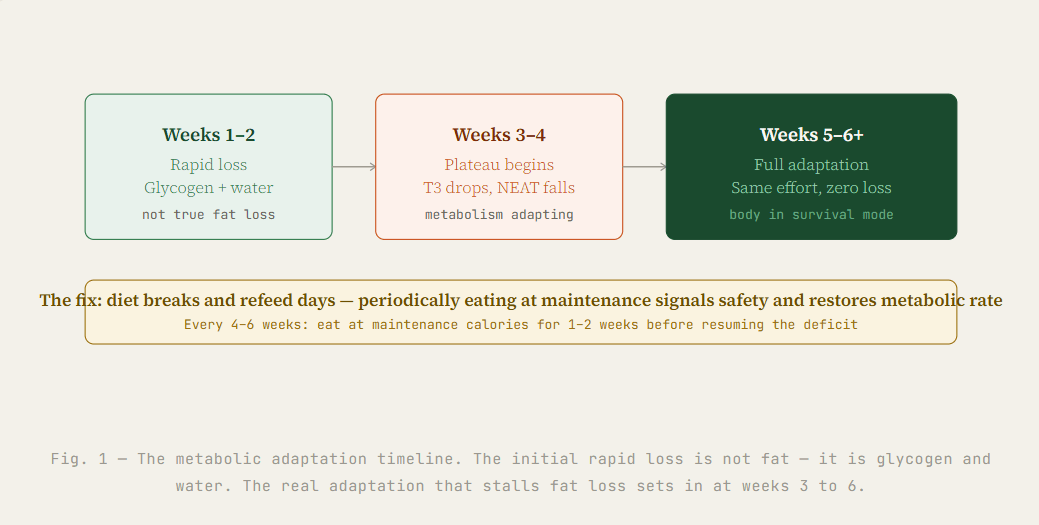
This is why people often lose weight quickly in the first two weeks and then nothing for the next month despite doing exactly the same things. The initial rapid loss was glycogen (stored carbohydrate) and water weight — your body depletes those first. The real metabolic adaptation sets in afterward.
How to break metabolic adaptation
The solution is counterintuitive but well-supported by research: eat more, periodically. Every 4 to 6 weeks of dieting, spend 1 to 2 weeks eating at your maintenance calories. This is called a diet break. It signals to your body that food is available, restores thyroid hormone production, and resets your metabolic rate before you return to a deficit. People who use planned diet breaks lose the same or more fat over 16 weeks compared to people who diet continuously — while preserving significantly more muscle mass.
Reason 2: You Are Eating More Than You Think
Calorie underestimation is the most common undiagnosed reason for failed fat loss, and it is not a character flaw. It is a predictable cognitive bias. Studies consistently show that people underestimate their calorie intake by 20 to 50%, with the highest underestimation occurring in people who believe they are eating carefully.
Why accurate tracking is harder than it looks
The mechanisms behind calorie blindness are specific and worth understanding. Cooking oils are the biggest hidden calorie source in most kitchens — a single tablespoon of oil contains 120 calories and it is very easy to use three to four tablespoons in a meal you believe is healthy. Restaurant portions are typically 30 to 50% larger than what nutrition databases list. Liquid calories — chai with two teaspoons of sugar three times a day, packaged fruit juice, flavoured yoghurt — accumulate to several hundred calories daily without registering as food to your brain.
The key variable that separates people who lose fat from people who plateau at the same effort level is almost always calorie tracking accuracy. This does not mean you must track every meal permanently — but tracking honestly for 2 to 3 weeks is the most useful diagnostic tool available to understand where your calories are actually going.
The exercise compensation trap: Research shows that people unconsciously eat more after exercise — sometimes more than the calories they burned. If you feel you have "earned" a larger meal after the gym, your body is doing exactly what evolution designed it to do. The brain registers calorie expenditure from exercise and increases appetite to compensate. This is why exercise alone produces much smaller weight loss than expected.
Reason 3: The Hidden Calorie Traps Specific to Indian Eating
Most fat loss articles are written for Western audiences eating Western food. If you are eating Indian food, there are specific calorie traps that generic advice completely misses — traps that look like healthy eating but silently eliminate your calorie deficit.
The roti plus rice combination
The traditional Indian thali — roti, rice, dal, and sabzi together in one meal — is nutritious and culturally important. For fat loss, however, eating both roti and rice in the same meal creates an extremely high carbohydrate load in a single sitting. When blood glucose rises sharply, insulin is released in quantity. Elevated insulin signals the body to store energy as fat and inhibits fat burning for the duration of the insulin response.
The fix is not to eliminate either food — it is to choose one per meal. Two rotis with dal, sabzi, and a protein source is a balanced meal. A small portion of rice with the same accompaniments is equally fine. Roti plus rice plus dal plus sabzi in one sitting is where the carbohydrate overload creates a fat loss problem.
India-specific context
The Indian cultural relationship with food means that eating less than what is served is often interpreted as disrespect or illness. Many people attempting fat loss eat appropriate portions at planned meals but then eat additional food at family meals to avoid conflict. This untracked eating is one of the most common reasons Indian clients plateau despite believing they are in a consistent deficit. If this applies to you, the solution is plate management — take a full plate, but load it heavily with sabzi and dal and use a smaller portion of roti or rice than usual. Nobody notices the plate composition.
The chai and snack calorie accumulation
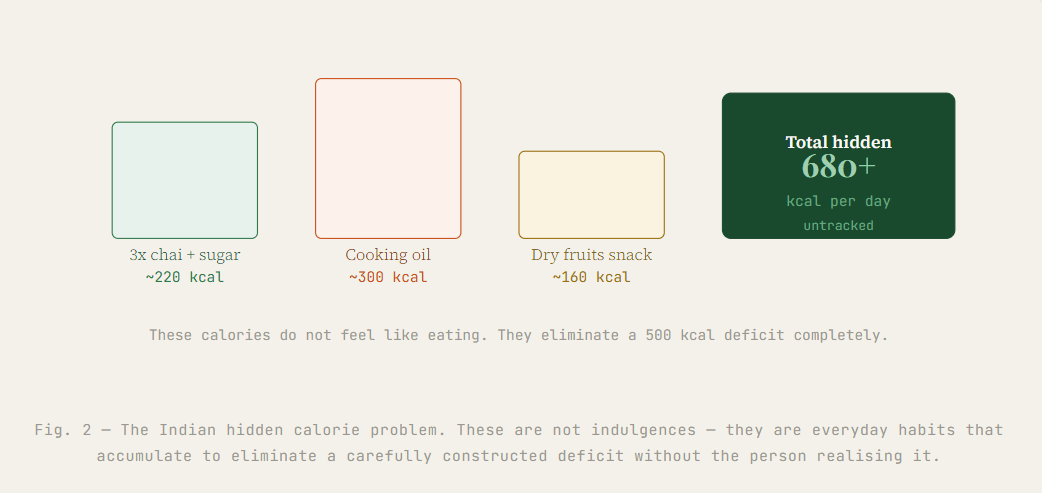
Three cups of chai daily with two teaspoons of sugar each and whole milk adds approximately 180 to 240 calories to your day — every day, invisibly, without feeling like food. Add the biscuits, mathri, or namkeen that accompany chai in most households and the invisible calorie addition rises to 350 to 500 calories daily. This alone can eliminate a carefully constructed calorie deficit entirely.
The mechanism is not the chai itself — it is the cognitive categorisation. Chai and its accompaniments are not mentally processed as food by most people. They are a social and cultural ritual. The calories are real regardless of how the food is categorised.
The healthy food portion problem
Nuts, dry fruits, ghee, coconut, and full-fat dairy are nutritionally excellent foods. They are also extremely calorie dense. A handful of mixed nuts is 160 to 200 calories. A tablespoon of ghee is 112 calories. When people switch from processed snacks to “healthy” Indian foods, they often increase total calories because they do not apply the same portion awareness to healthy foods that they would to an obvious indulgence.
Reason 4: You Are Doing the Wrong Type of Exercise for Fat Loss
Running on the treadmill every day is better than sitting on the sofa. But cardio-only exercise is one of the least efficient fat loss strategies available, and doing more of it when fat loss stalls is one of the most common mistakes people make. The mechanism behind why resistance training beats cardio for long-term fat loss is specific and important to understand.
Why cardio alone does not sustain fat loss
Cardio burns calories during the activity. When you stop, the calorie burn stops. Over time, your body adapts to cardio by becoming more efficient — it learns to perform the same movement using fewer calories. A 45-minute run that burned 400 calories in week one burns 320 calories in week eight as your cardiovascular system and muscles adapt. You are working the same amount, burning progressively less.
Resistance training works differently. When you build muscle through weight training, you increase your resting metabolic rate permanently — muscle tissue burns 3 times more calories at rest than fat tissue. A person who adds 2 kg of muscle burns an additional 60 to 80 calories per day without doing anything extra. Over a month that is 1,800 to 2,400 additional calories burned — equivalent to 4 to 5 extra gym sessions.
The NEAT reduction problem
Non-exercise activity thermogenesis — the calories you burn through unconscious movement like fidgeting, posture, walking around the house, gesturing while talking — drops significantly when you are in a calorie deficit. This is another metabolic adaptation mechanism. When your body senses energy restriction, it conserves energy by making you move less unconsciously. People in a deficit often sit more, gesticulate less, and generally reduce their total daily movement outside of planned exercise without realising it. This can account for a reduction of 200 to 400 calories per day from total energy expenditure.
The resistance training minimum that makes a difference: Two sessions per week of compound resistance training — squats, deadlifts, rows, pressing movements — targeting all major muscle groups is the minimum effective dose for metabolic benefit. You do not need to become a bodybuilder. You need to maintain and build muscle mass enough to keep your resting metabolic rate from dropping during a fat loss phase.
Reason 5: Your Hormones Are Actively Blocking Fat Loss
Hormones are the master controllers of fat storage and fat burning. When they are dysregulated — from insulin resistance, thyroid issues, PCOS, or chronically elevated cortisol — the body can be physiologically locked into fat storage mode regardless of diet and exercise. This is not excuses. It is endocrinology.
Insulin resistance and fat storage
Insulin is the hormone that controls whether glucose from food is used as energy or stored as fat. In a healthy insulin-sensitive person, insulin rises after a meal, glucose is delivered to cells for energy, and insulin returns to baseline quickly. In insulin-resistant individuals, cells stop responding properly to insulin signals. The pancreas responds by producing more insulin to compensate. Chronically elevated insulin keeps the body in fat storage mode — it directly inhibits the enzyme that releases fat from storage (hormone-sensitive lipase) — making fat loss very difficult even in a calorie deficit.
Insulin resistance is extremely common in India due to a combination of genetic predisposition to central fat storage, high refined carbohydrate diets, physical inactivity, and metabolic syndrome patterns. Signs include difficulty losing weight especially around the abdomen, sugar cravings after meals, energy crashes 1 to 2 hours after eating, and darkening of skin in the neck folds or armpits (acanthosis nigricans).
PCOS and hormonal fat storage
Polycystic ovary syndrome affects an estimated 1 in 5 Indian women, making it one of the most common reasons women struggle with fat loss despite genuine effort. PCOS creates a triple hormonal problem for fat loss: elevated androgens promote central fat storage, insulin resistance makes the body store more glucose as fat, and disrupted LH/FSH ratios affect overall metabolic function. Women with PCOS often need a specifically different strategy — lower glycaemic load meals, higher protein intake, resistance training prioritised over cardio, and in some cases medical management of insulin resistance — rather than just a standard calorie deficit.
India-specific context
Thyroid disorders — particularly hypothyroidism — are significantly more common in India than global averages suggest, with studies indicating prevalence of 10 to 11% in Indian adults versus 4 to 5% globally. An underactive thyroid directly reduces metabolic rate and causes weight gain or failure to lose weight despite diet and exercise. If you have been consistently in a deficit and exercising for more than 3 months without measurable fat loss, getting thyroid function tested (TSH, T3, T4) is a straightforward diagnostic step worth taking.
Reason 6: Poor Sleep Is Destroying Your Fat Loss Hormones
Sleep is not rest from fat loss. It is when the most critical fat loss hormones are regulated. Getting less than 7 hours of sleep consistently creates a hormonal environment that makes fat loss physiologically difficult — not just harder, but genuinely impaired at a biological level.
The ghrelin and leptin mechanism
Two hormones directly control hunger and satiety. Ghrelin signals hunger — the more ghrelin, the hungrier you feel. Leptin signals fullness — the more leptin, the more satisfied you feel after eating. A single night of sleeping less than 6 hours increases ghrelin by 14.9% and decreases leptin by 15.5%. This means you wake up meaningfully hungrier than usual and feel less full after eating the same amount of food. Over a week of poor sleep, this creates a consistent daily calorie surplus that easily eliminates any deficit you are trying to maintain through conscious effort.
The sleep → fat loss mechanism
Less than 7 hours sleep → ghrelin rises by ~15%, leptin falls by ~15% → you eat more the next day without realising it → cortisol also rises from sleep deprivation → elevated cortisol promotes abdominal fat storage → fat loss stalls or reverses despite same diet and exercise
The cortisol connection
Sleep deprivation raises cortisol — the primary stress hormone. Elevated cortisol signals the body to store fat, particularly visceral fat around the abdomen. It also promotes muscle breakdown, which reduces resting metabolic rate. And it increases cravings specifically for high-calorie, high-fat, high-sugar foods — the exact foods most people are trying to avoid when dieting.
In Indian urban contexts — late-night mobile phone use, early morning commutes, work demands, disrupted circadian rhythms from irregular meal timing — chronic sleep deprivation is extremely common. Many people sleeping 5 to 6 hours per night attribute their lack of fat loss to diet and exercise problems when the root cause is hormonal disruption from insufficient sleep.
The practical threshold: Research consistently shows that 7 to 8 hours of sleep per night is the minimum for normal ghrelin and leptin regulation. Below 6 hours, the hormonal disruption is significant enough to meaningfully impair fat loss independent of diet and exercise quality. If you are consistently sleeping under 6 hours, addressing sleep before further restricting food or increasing exercise will produce better results.
Reason 7: The Scale Is Measuring the Wrong Thing
The scale measures total body mass — fat, muscle, water, bone, the contents of your digestive tract. It cannot distinguish between fat loss and muscle gain. It cannot separate water retention from fat accumulation. Many people who are making excellent body composition progress quit because the scale is not moving, when in reality they are losing fat and gaining muscle simultaneously.
Why body composition change is not visible on the scale
Muscle tissue is denser than fat tissue — it weighs approximately 18% more per unit of volume. This means that when you add muscle and lose fat, your body can become visibly leaner and your clothes can fit better while your scale weight stays exactly the same or even increases slightly. This is particularly common in the first 8 to 12 weeks of a new resistance training programme when muscle protein synthesis is highest.
Water retention also masks fat loss on the scale. Carbohydrate-containing food stores water — each gram of glycogen holds approximately 3 grams of water. When you eat more carbohydrates than usual (after a function, during a festival, on a cheat meal), your scale weight can increase by 1 to 2 kg overnight from water retention alone. This is not fat gain. The water releases within 2 to 3 days when carbohydrate intake returns to normal.
Better measurements than scale weight
Waist circumference measured at the navel every two weeks is a more accurate indicator of fat loss than scale weight — particularly for visceral fat reduction which is the most health-significant type. Progress photos taken in consistent lighting and posture every 4 weeks show body composition changes the scale cannot capture. How your clothes fit — particularly at the waist — is often the most honest daily indicator of direction of travel.
What to Do When Fat Loss Has Stalled: A Practical Protocol
Rather than trying everything at once, the most effective approach to breaking a plateau is diagnosing which specific mechanism is causing your stall and addressing that first. Most people are dealing with two or three of the above reasons simultaneously — fixing the most impactful one first creates visible progress that motivates addressing the others.
The diagnostic sequence
Step 1 — Track calories honestly for 7 days. Use any calorie tracking app and measure everything including oils, chai, and condiments. If your tracked intake is more than 200 calories above where you thought you were eating, calorie blindness is your primary problem. Fix that first.
Step 2 — Assess your sleep. Are you consistently getting 7 or more hours? If not, prioritise this before any other change. The hormonal improvement from adequate sleep will produce more fat loss improvement than any dietary tweak you can make while running on 5 hours.
Step 3 — Check your exercise type. Are you doing any resistance training? If not, add two sessions per week. Are you doing only the same cardio workout every time? Introduce variety and progressive overload.
Step 4 — Consider a diet break. If you have been in a consistent calorie deficit for 6 or more weeks without a break, spend 1 to 2 weeks eating at maintenance. Then return to your deficit. Many people find that the plateau breaks in the first week back on the deficit after a diet break.
Step 5 — Consider getting bloodwork done. If you have addressed all of the above for 4 to 6 weeks and fat loss still has not resumed, thyroid function, fasting insulin, and for women — testosterone and LH/FSH levels — are worth testing. These are not exotic tests. Any GP can order them.
faq
Daily exercise without weight loss is usually caused by one of three mechanisms: metabolic adaptation (your body burns fewer calories as you get fitter), compensatory eating (you unconsciously eat more after workouts), or doing only cardio without resistance training (which prevents the muscle mass that drives resting metabolism). Exercise is necessary but cannot create a fat loss environment alone — diet quality and hormonal balance matter equally.
Eating less without losing weight is typically caused by metabolic adaptation — your body reduces its calorie burn to match your reduced intake. If you cut calories too aggressively, cortisol rises, muscle breaks down, and resting metabolic rate drops. The solution is not to eat even less, but to break the adaptation by periodically cycling calories upward, adding resistance training to protect muscle mass, and addressing sleep and stress which directly control fat storage hormones.
Most people see measurable fat loss changes in 4 to 6 weeks if calorie deficit, protein intake, sleep, and stress are all optimised together. The first 1 to 2 weeks often show rapid water weight loss that then stalls — this is not fat loss plateauing, it is the body depleting glycogen stores. True fat tissue loss requires sustained consistency over 6 to 12 weeks for visible changes in body composition.
Yes. Roti and rice are not inherently fattening. They become a fat loss problem when portions are large, when they are eaten without adequate protein, or when they are combined in the same meal creating a very high carbohydrate load. The fix is not eliminating them but structuring meals with protein first — dal, eggs, paneer, chicken — and treating roti or rice as a side rather than the base of the meal.
Yes, chronically elevated cortisol from stress directly blocks fat loss by shifting the body into fat storage mode, particularly around the abdomen. Cortisol also increases appetite and cravings for high-calorie foods. In Indian urban contexts — long commutes, work pressure, disrupted sleep — cortisol levels are chronically elevated in many people, making fat loss physiologically difficult regardless of diet and exercise quality.
Losing inches while the scale stays flat is a sign that your body is simultaneously losing fat and gaining muscle — a highly desirable body composition change. Muscle is denser than fat, meaning the same volume of muscle weighs more. This is especially common in the first 8 to 12 weeks of a new resistance training programme. The scale measures total mass and cannot distinguish between fat loss and muscle gain. Measure waist circumference and how clothes fit for more accurate progress tracking.
PCOS creates insulin resistance which makes fat loss significantly harder by causing the body to store more blood sugar as fat rather than using it for energy. Women with PCOS often need to prioritise lower glycaemic load meals, higher protein intake, and resistance training specifically — not just calorie restriction — to manage insulin sensitivity and create the hormonal environment for fat loss.
Summary
Not losing weight despite exercise and diet is almost always a biology problem, not a willpower problem. The seven mechanisms most commonly responsible are metabolic adaptation to sustained calorie restriction, calorie underestimation especially from cooking oils and chai, specific Indian dietary patterns that create carbohydrate overload, cardio-only exercise that does not build metabolically active muscle, insulin resistance or thyroid dysfunction, sleep deprivation disrupting ghrelin and leptin, and scale weight that does not reflect true fat loss because of simultaneous muscle gain.
The most important principle for breaking a plateau is diagnosis before action. Identify which mechanism is causing your specific stall before changing anything. More restriction is rarely the answer — smarter strategy almost always is.
If you have been consistent for more than 3 months without progress despite addressing diet, exercise, and sleep, get bloodwork done. Thyroid, fasting insulin, and for women — hormone panels — are straightforward tests that can identify a physiological barrier that no amount of diet and exercise will overcome without medical management.
Your body is not broken. It is doing exactly what it is designed to do. Understanding the mechanism gives you the power to work with your biology instead of against it.
Medical disclaimer: This article provides science-based general information for educational purposes. It is not a substitute for personalised medical advice. If you have a medical condition such as PCOS, thyroid disorder, or diabetes that may be affecting your weight, consult a qualified doctor or registered dietitian before making significant changes to your diet or exercise programme.